
Findings

Conclusion
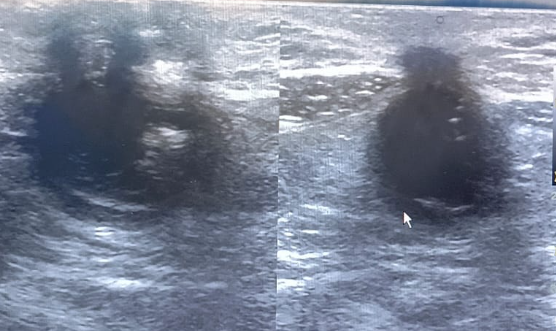
📋 Findings suggest an inflamed umbilical-urachal sinus with preperitoneal abscess formation.
Recommendation: CT Abd. follow-up.
Causes of Umbilical-Urachal Sinus with Abscess
- Persistent Urachus: Congenital failure of the urachus to completely obliterate after birth.
- Infection of the urachal remnant from:
- Skin flora or urinary tract pathogens
- Poor umbilical hygiene or trauma
- Secondary Bacterial Invasion of sinus tract → Abscess formation in the preperitoneal space (between the peritoneum and anterior abdominal wall).
Symptoms
- Umbilical Discharge: Purulent, foul-smelling
- Lower Abdominal Pain: Especially in the suprapubic region
- Redness and Swelling: Around the umbilicus
- Fever and Malaise: Systemic signs of infection
- Tender Mass: Palpable in lower midline abdomen (preperitoneal abscess)
- Occasionally: Dysuria or urinary symptoms if bladder is involved
Diagnosis
- Clinical Examination
- Inspect umbilicus for discharge or redness
- Palpate for tenderness or mass in suprapubic area
- Ultrasound (First-line Imaging)
- Hypoechoic or complex collection in preperitoneal space
- Tubular hypoechoic tract from umbilicus toward bladder (urachal sinus)
- Surrounding fat stranding indicates inflammation
- CT Abdomen/Pelvis with Contrast
- Better defines extent of abscess
- Identifies communication with bladder or peritoneum
- Helpful for pre-surgical planning
- Laboratory Tests
- ↑ WBC count, CRP (infection markers)
- Pus culture if discharge present
- Urinalysis to rule out associated UTI
This MCQ is for you: Drop your answer in the comment box below, then click the button to reveal the answer key.
1. Which of the following best describes an umbilical-urachal sinus?
A. A patent connection between bladder and umbilicus
B. A midline cyst within the urachal tract
C. A blind-ending tract extending from the umbilicus
D. A diverticulum extending from the posterior bladder wall
👉 Explanation: A urachal sinus is an incomplete closure of the urachus, leaving a blind-ending tract from the umbilicus without communication to the bladder.
2. What is the most common clinical presentation of an infected umbilical-urachal sinus?
A. Hematuria
B. Umbilical discharge and suprapubic pain
C. Gross abdominal distension
D. Painless hematuria
👉 Explanation: Infected urachal sinuses commonly present with purulent umbilical discharge and localized suprapubic discomfort or swelling.
3. Which imaging modality is most commonly used first to evaluate suspected urachal abnormalities?
A. MRI abdomen
B. Intravenous pyelogram
C. Ultrasound abdomen
D. X-ray abdomen
👉 Explanation: Ultrasound is non-invasive, cost-effective, and typically the first imaging modality to detect fluid collections or sinus tracts in urachal anomalies.
4. The urachus is embryologically derived from which structure?
A. Mesonephric duct
B. Cloaca
C. Allantois
D. Ureteric bud
👉 Explanation: The urachus develops from the allantois, a structure involved in early fetal waste removal that typically regresses after birth.
5. A key ultrasound finding in a urachal sinus with abscess is:
A. Hyperechoic linear band along the bladder wall
B. Hypoechoic tubular tract extending from umbilicus
C. Anechoic fluid in the Morrison’s pouch
D. Calcified lesion in the kidney
👉 Explanation: A hypoechoic or complex tubular tract running from the umbilicus toward the bladder is characteristic of a urachal sinus.
6. The definitive treatment for an umbilical-urachal sinus complicated by abscess is:
A. Only oral antibiotics
B. Needle aspiration and watchful waiting
C. Surgical excision of the tract with drainage
D. Umbilical hernia repair
👉 Explanation: Complete surgical excision of the urachal tract along with drainage of any abscess is essential to prevent recurrence and complications.
7. What is the typical location of a urachal abscess on imaging?
A. Retroperitoneal space
B. Right lower quadrant
C. Between the umbilicus and bladder in the preperitoneal space
D. Left hypochondrium
👉 Explanation: The urachus lies in the midline, between the peritoneum and transversalis fascia, making the preperitoneal space the common abscess site.
8. Which laboratory finding is most commonly associated with an infected urachal sinus?
A. Decreased hemoglobin
B. Elevated creatinine
C. Leukocytosis with raised CRP
D. Hypokalemia
👉 Explanation: Infection typically causes a systemic inflammatory response with elevated white blood cells and C-reactive protein.
9. What complication may arise if an infected urachal sinus is left untreated?
A. Spontaneous bladder rupture
B. Peritonitis or sepsis
C. Pulmonary embolism
D. Appendicitis
👉 Explanation: Infections from the urachal sinus can spread into surrounding tissues or the peritoneal cavity, causing sepsis or peritonitis.
10. The urachus is anatomically located in which structure?
A. Retropubic space
B. Median umbilical ligament
C. Round ligament of liver
D. Inguinal canal
👉 Explanation: The median umbilical ligament is the fibrous remnant of the urachus extending from the bladder apex to the umbilicus.
11. Which age group most commonly presents with urachal anomalies?
A. Neonates
B. Children under 5 years
C. Adolescents
D. Infants and young children, but may remain undiagnosed until adulthood
👉 Explanation: Although congenital, urachal anomalies may remain asymptomatic and present later in childhood or even adulthood if infected.
12. On CT imaging, which of the following is most likely seen in a complicated urachal sinus?
A. Calcified mass within the liver
B. A fluid-filled midline tract with surrounding fat stranding
C. Intravesical air-fluid level
D. Bilateral ureteral dilation
👉 Explanation: CT clearly shows a midline tubular lesion with inflammation, which is useful for preoperative planning and detecting abscesses.
13. Which of the following is NOT a typical symptom of urachal abscess?
A. Umbilical discharge
B. Suprapubic pain
C. Fever
D. Hematuria as the only finding
👉 Explanation: Hematuria is more typical of urachal cysts or carcinomas that communicate with the bladder, not commonly in infected sinuses.
14. What is the embryological fate of the urachus under normal development?
A. Converts into the falciform ligament
B. Becomes the median umbilical ligament
C. Becomes the inferior epigastric artery
D. Persists as a functional tract
👉 Explanation: Normally, the urachus involutes to become a fibrous cord—the median umbilical ligament—by birth.
15. Which bacteria are commonly implicated in urachal sinus infection?
A. E. coli and Staphylococcus aureus
B. Listeria and Salmonella
C. Pseudomonas and Klebsiella
D. Chlamydia and Neisseria gonorrhoeae
👉 Explanation: The most common pathogens are skin and gut flora such as E. coli and Staph. aureus, especially in infected sinuses.
1. निम्नलिखित में से उम्बिलिकल-यूरैकल साइनस का सर्वोत्तम वर्णन क्या है?
A. मूत्राशय और नाभि के बीच एक खुला संपर्क
B. यूरैकल पथ के भीतर एक मिडलाइन सिस्ट
C. नाभि से शुरू होकर बंद होने वाली एक ट्यूब जैसी संरचना
D. मूत्राशय की पिछली दीवार से निकला एक डायवर्टीकुलम
Explanation: यह एक अपूर्ण रूप से बंद यूरैकस होता है, जो नाभि से शुरू होकर एक बंद साइनस बनाता है।
2. एक संक्रमित यूरैकल साइनस की सबसे आम नैदानिक प्रस्तुति क्या है?
A. पेशाब में खून
B. नाभि से मवाद का रिसाव और अधनाभि दर्द
C. पेट का अत्यधिक फूला होना
D. दर्द रहित हेमेचूरिया
Explanation: रोगी में आमतौर पर नाभि से बदबूदार स्राव और अधनाभि क्षेत्र में दर्द व सूजन होती है।
3. यूरैकल असामान्यता की पहचान के लिए सबसे पहले कौन सी इमेजिंग तकनीक उपयोग की जाती है?
A. MRI
B. इंट्रावेनस पाइलोग्राम
C. अल्ट्रासाउंड
D. एक्स-रे
Explanation: अल्ट्रासाउंड एक सरल, सस्ता और प्रभावी प्रारंभिक परीक्षण है।
4. यूरैकस भ्रूण में किस संरचना से विकसित होता है?
A. मेसोनेफ्रिक डक्ट
B. क्लोअका
C. एलेनटोइस
D. यूरेटरिक बड
Explanation: यूरैकस भ्रूणीय एलेनटोइस से विकसित होता है, जो जन्म के बाद सामान्यतः फाइब्रस लिगामेंट बन जाता है।
5. अल्ट्रासाउंड में यूरैकल साइनस के साथ एब्सेस का एक मुख्य लक्षण क्या होता है?
A. मूत्राशय की दीवार पर हाइपरेकोइक बैंड
B. नाभि से मूत्राशय की ओर जाता हाइपोइकोइक ट्यूब
C. मॉरिसन पाउच में तरल पदार्थ
D. गुर्दे में कैल्सिफाइड लक्षण
Explanation: नाभि से मूत्राशय की दिशा में फैला हाइपोइकोइक ट्रैक यूरैकल साइनस की पहचान करता है।
6. संक्रमित यूरैकल साइनस के लिए अंतिम और प्रभावी उपचार क्या है?
A. केवल मौखिक एंटीबायोटिक
B. सुई द्वारा एस्पिरेशन
C. सर्जिकल ट्रैक एक्सिशन और एब्सेस ड्रेनेज
D. नाभि हर्निया सर्जरी
Explanation: संक्रमण के बाद यूरैकल ट्रैक को पूरी तरह से निकालना और एब्सेस को साफ करना आवश्यक होता है।
7. इमेजिंग में यूरैकल एब्सेस आमतौर पर किस स्थान पर पाया जाता है?
A. रेट्रोपेरिटोनियल स्पेस
B. दाहिने निचले हिस्से में
C. नाभि और मूत्राशय के बीच प्रीपेरिटोनियल स्पेस में
D. बाएं ऊपरी हिस्से में
Explanation: यूरैकस नाभि और मूत्राशय के बीच मिडलाइन में प्रीपेरिटोनियल स्पेस में स्थित होता है।
8. संक्रमित यूरैकल साइनस से संबंधित सबसे सामान्य लैब रिपोर्ट क्या दिखाती है?
A. कम हीमोग्लोबिन
B. बढ़ा हुआ क्रिएटिनिन
C. ऊंचा WBC और CRP
D. कम पोटैशियम
Explanation: यह संक्रमण का संकेत है और शरीर की प्रतिरक्षा प्रतिक्रिया दर्शाता है।
9. यदि संक्रमित यूरैकल साइनस का समय पर इलाज न किया जाए, तो क्या जटिलताएँ हो सकती हैं?
A. मूत्राशय का फटना
B. पेरिटोनाइटिस या सेप्सिस
C. पल्मोनरी एम्बोलिज्म
D. अपेंडिसाइटिस
Explanation: संक्रमण फैलकर पूरे शरीर में गंभीर समस्याएं पैदा कर सकता है।
10. यूरैकस शरीर में किस संरचना के रूप में स्थित होता है?
A. रेट्रोप्यूबिक स्पेस
B. मीडियन अम्बिलिकल लिगामेंट
C. राउंड लिगामेंट ऑफ लिवर
D. इनगुइनल कैनाल
Explanation: यूरैकस जन्म के बाद एक फाइब्रस लिगामेंट में परिवर्तित हो जाता है जो मीडियन अम्बिलिकल लिगामेंट कहलाता है।
11. यूरैकल असामान्यताएँ आमतौर पर किस आयु वर्ग में देखी जाती हैं?
A. नवजात
B. 5 वर्ष से कम बच्चे
C. किशोर
D. शिशु और बच्चे, लेकिन कभी-कभी वयस्कों में भी
Explanation: यूरैकल डिफेक्ट्स जन्म से होते हैं लेकिन लक्षण बड़े होने पर सामने आ सकते हैं, खासकर संक्रमण होने पर।
12. CT स्कैन में जटिल यूरैकल साइनस के लक्षण क्या होते हैं?
A. लिवर में कैल्सिफाइड मास
B. मिडलाइन में तरल से भरा ट्रैक और आसपास की सूजन
C. मूत्राशय के अंदर हवा और तरल का स्तर
D. दोनों यूरेटर का फैलाव
Explanation: CT स्कैन ट्रैक और सूजन को स्पष्ट रूप से दिखाता है, और सर्जरी की योजना बनाने में मदद करता है।
13. निम्न में से कौन सा लक्षण यूरैकल एब्सेस में आमतौर पर नहीं पाया जाता?
A. नाभि से स्राव
B. अधनाभि दर्द
C. बुखार
D. केवल हेमेचूरिया
Explanation: केवल हेमेचूरिया आमतौर पर यूरैकल ट्यूमर या सिस्ट में देखा जाता है, न कि संक्रमण में।
14. सामान्य भ्रूण विकास के दौरान यूरैकस का क्या होता है?
A. फाल्सीफॉर्म लिगामेंट बन जाता है
B. मीडियन अम्बिलिकल लिगामेंट में परिवर्तित होता है
C. इन्फीरियर एपिगैस्ट्रिक धमनी बनता है
D. जन्म के बाद भी कार्यात्मक रहता है
Explanation: जन्म से पहले यूरैकस फाइब्रस होकर मीडियन अम्बिलिकल लिगामेंट में बदल जाता है, जो सामान्य प्रक्रिया है।
15. यूरैकल साइनस के संक्रमण में आम तौर पर कौन से बैक्टीरिया पाए जाते हैं?
A. E. coli और Staphylococcus aureus
B. Listeria और Salmonella
C. Pseudomonas और Klebsiella
D. Chlamydia और Neisseria gonorrhoeae
Explanation: यूरैकल संक्रमण में आमतौर पर त्वचा और आंत्र जीवाणु जैसे E. coli और Staph aureus शामिल होते हैं।
📘 उत्तर कुंजी (Answer Key)
यह उत्तर तालिका केवल सब्सक्राइब करने के बाद दिखाई देगी।
This answer key will be visible only after you subscribe.
कृपया नीचे क्लिक करके हमारे ब्लॉग को सब्सक्राइब करें:
Please click below to subscribe to our blog:















