Normal Late first trimester ultrasound survey A Normal Late First Trimester Ultrasound Survey typically occurs between 11 to 13.6 weeks of gestation. It is an important diagnostic tool that assesses fetal development and screens for potential abnormalities. The key components of a normal survey during this stage include: Fetal Structures Assessed in the Late First Trimester (11w to 13w 6d) 1– Structures of neutral Positions of the Fetus 2– Cranial Structures 3–Facial Structures 4–Neck Structures 5–Thoracic Structures 6–Abdominal Structures 7–Limbs and Extremities 8–Spine 9–Genitourinary System 10– Placenta 11–Umbilical Cord 12– Amniotic Fluid Assessment 13– Maternal Anatomy Assessment 1. Structures of neutral Positions of the Fetus
A neutral position in fetal ultrasound refers to a standardized orientation of specific anatomical structures to ensure accurate measurement and assessment. This position is essential for reducing variability in measurements, particularly during the late first trimester.
The fetal head should be in a neutral or slightly flexed position, neither excessively flexed (chin too close to the chest) nor hyperextended (head tilted backward).
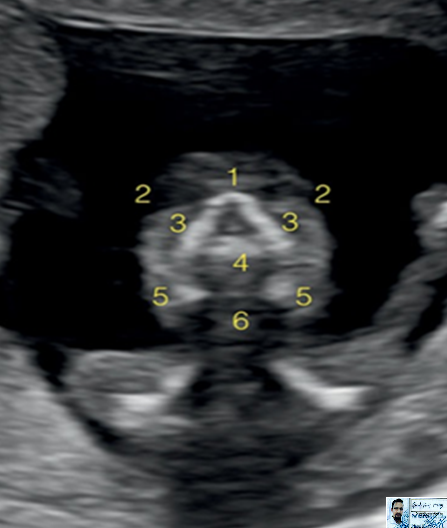
Cranial Structures
1-NT 2-Nasal bone 3-Maxilla 4-Mandible 5-Thalamus 6-Brain stem 7-Fourth ventricle 8-Choroid plexus 9-Cisterna magna
Normal first trimester ultrasound survey Understand critical signs, scan parameters, and interpretation tips. Ideal for OB-GYN and radiology learners. The first trimester of pregnancy (Less than 13w) is a critical period of development, during which the embryo progresses to a fetus. Here’s an overview of the normal anatomy observed during this stage:Early first trimester structure (Less than 10w 06d) 1– Intradecidual Sac Sign (IDSS)/Very early pregnancy 2– Gestational Sac 3– Yolk Sac 4– Amnion 5– Fetal Pole 6– Cardiac Activity 7– Omphalomesenteric duct or vitelline duct 8– Placenta 9– Uterus and Adnexa 10– Timeline of fetal structure appears in ultrasound TAS/TVS 11– Differences in Detection: TAS vs TVS
1– Intradecidual Sac Sign (IDSS)/Very early pregnancy
The intradecidual sac sign (IDSS) is one of the earliest ultrasound findings suggestive of an intrauterine pregnancy (IUP). It helps distinguish an early intrauterine gestational sac from a potential ectopic pregnancy.
The IDSS appears as a small, round, anechoic (fluid-filled) structure within the decidua of the endometrial cavity, but not in the central endometrial stripe.
It is typically seen as early as 4 to 4.5 weeks of gestation on transvaginal ultrasound (TVUS).
The sac is located eccentrically, meaning it is implanted within one side of the thickened decidua rather than in the middle
Significance:
Early indicator of intrauterine pregnancy (IUP): The IDSS is considered an early sign before the yolk sac and fetal pole become visible.
Distinguishing from pseudogestational sac: Unlike a central fluid collection seen in ectopic pregnancies (pseudogestational sac), the true gestational sac appears eccentric in location with a surrounding echogenic rim.
Confirmation needed: IDSS alone is not definitive for a viable pregnancy and should be followed up with serial ultrasounds to confirm the presence of a yolk sac, fetal pole, and cardiac activity.
2– Gestational Sac
The first identifiable structure on ultrasound, typically visible by 4.5 to 5 weeks via transvaginal ultrasound and in trans abdominal at 5 weeks 1 day of conception
Located in the fundal or mid-uterine cavity.
Grows approximately 1 mm per day.
3– Yolk Sac
Appears within the gestational sac around 5 weeks.
Provides early nutrition and contributes to blood cell formation.
Should be ≤ 6 mm; a larger size may indicate abnormal pregnancy.
4– Amnion The amnion is the thin, inner fetal membrane that encloses the amniotic cavity, which contains the amniotic fluid and surrounds the developing embryo/fetus.
It plays a vital role in:
The amnion early appears at 7w in sonogram.
Providing a protective fluid environment.
Allowing fetal movement and growth.
Preventing adhesions between the embryo and surrounding structures.
Serving as a barrier against infections.
5– Fetal Pole
Visible by 5.5 to 6 weeks on transvaginal ultrasound.
Grows at approximately 1 mm per day.
Crown-rump length (CRL) is used to estimate gestational age.
Cardiac activity should be present by 6 weeks (normal heart rate: 100–180 bpm).
6– Cardiac Activity Early cardiac pulsation appears 5w 6D to 6w 3D.
M-mode ultrasound shows a heart rate of 111 beats/min of 6w 6D embryo.
7– Omphalomesenteric duct or vitelline duct
The omphalomesenteric duct (OMD), also known as the vitelline duct, is an embryological structure that connects the midgut to the
yolk sac. Early appears at 6w.
Begins forming around 5–6 weeks.
Initially short, later elongates with twisting due to fetal movements.
Contains two arteries and one vein.
8– Placenta
The placenta early appears in 8-9weeks of gestation
9– Uterus and Adnexa Uterus: Normal size and echotexture
Ovaries: Right ___ / Left ___ (corpus luteum, cysts if any)
Adnexa: No adnexal masses
Free Fluid: None / Minimal physiological
10– Timeline of fetal structure appears in ultrasound TAS/TVS
Gestational Age (GA)
Structure Seen
Transvaginal Scan (TVS)
Transabdominal Scan (TAS)
3.5–4 weeks
Endometrial decidual reaction
Yes
Rare
4–4.5 weeks
Gestational sac (GS)
Visible (2–3 mm)
Difficult to see
5.0 weeks
Yolk sac (within GS)
Seen clearly
May be faint or absent
5.5–6.0 weeks
Fetal pole
Detectable
Often not seen
6.0 weeks
Cardiac activity (flicker)
Yes (with fetal pole)
⚠ Often missed
6.5–7.0 weeks
Embryo length (CRL measurable)
Clearly seen
May be difficult
7–8 weeks
Amniotic sac, head-body differentiation
Good detail
Limited view
8–9 weeks
Limb buds, developing brain vesicles
Yes
Possibly visible
9–10 weeks
Facial features, limb movement, spinal outline
Yes
Yes
11–13+6 weeks
NT, nasal bone, detailed anatomy survey
Excellent resolution
Adequate for screening
Notes: 1–TVS is more sensitive and should be used for early pregnancy Less than 8 weeks. 2– TAS is better after the bladder is full and GA is >7 weeks. 3– Cardiac activity should be confidently detected by 6.0–6.3 weeks (TVS). 4– If no fetal pole by MSD ≥25 mm or no cardiac activity in CRL ≥7 mm consider nonviability [based on current ACOG (American College of Obstetricians and Gynecologists) criteria].